Tennis players rely on one joint more than almost any other athlete—the shoulder. Every serve, overhead smash, and high forehand places tremendous stress on the rotator cuff. When that system begins to fail, even simple activities like reaching into a cabinet or sleeping on one side can become painful.
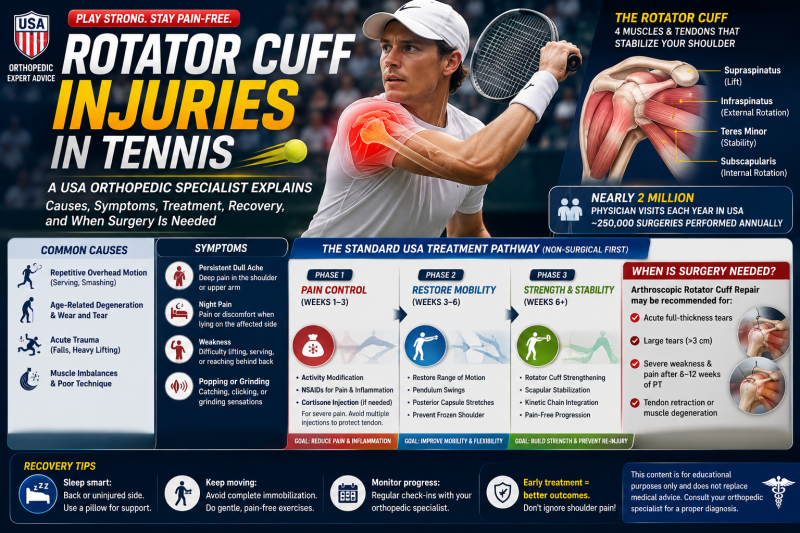
According to the American Academy of Orthopaedic Surgeons (AAOS) and other major U.S. orthopedic organizations, rotator cuff disorders are among the most common causes of shoulder pain, leading to nearly 2 million physician visits annually in the United States. Approximately 250,000 Americans undergo rotator cuff repair surgery each year, making it one of the most frequently performed orthopedic procedures.
For tennis players, understanding this injury can mean the difference between returning to the court successfully and developing a chronic shoulder problem.
Why Tennis Players Are at High Risk
The shoulder is the most mobile joint in the human body.
Unlike the hip, which has a deep socket for stability, the shoulder sacrifices stability to achieve tremendous freedom of movement.
This allows tennis players to generate explosive serves exceeding 120 mph, powerful overheads, and aggressive topspin forehands.
However, that mobility comes with a price.
Every overhead stroke places repeated stress on the tendons that stabilize the shoulder.
Thousands of serves each year can gradually overload these structures, especially if technique, strength, or recovery are inadequate.
Understanding the Rotator Cuff
The rotator cuff consists of four muscles and their tendons that work together to stabilize the shoulder joint:
- Supraspinatus – assists with lifting the arm.
- Infraspinatus – helps rotate the arm outward.
- Teres Minor – contributes to external rotation and stability.
- Subscapularis – rotates the arm inward and supports shoulder control.
Together, these muscles keep the upper arm centered in the shoulder socket during every tennis stroke.
When one tendon becomes damaged, the entire movement system can become less efficient and more painful.
Acute vs. Degenerative Tears
Orthopedic specialists generally classify rotator cuff injuries into two main categories.
Acute Tears
Acute tears occur suddenly.
Common causes include:
- Falling on an outstretched arm.
- Lifting a heavy object unexpectedly.
- A violent tennis serve or overhead smash.
- Shoulder dislocation.
- Direct trauma during sports.
Patients often describe a sudden sharp pain accompanied by immediate weakness.
Degenerative Tears
Degenerative tears develop gradually.
These are particularly common in adults over 40 and may result from:
- Years of repetitive overhead sports.
- Age-related tendon wear.
- Reduced blood supply to the tendon.
- Chronic inflammation.
- Repeated microtrauma.
Many tennis players notice symptoms developing slowly over months rather than after one specific injury.
Partial vs. Full-Thickness Tears
Doctors also classify tears based on severity.
Partial-Thickness Tear
The tendon is damaged but remains attached.
The Ellman Classification grades partial tears according to depth:
- Grade I – mild.
- Grade II – moderate.
- Grade III – greater than 50% of tendon thickness.
Many recreational tennis players fall into this category.
Full-Thickness Tear
A complete tear means the tendon has separated from the bone.
Without treatment, the tendon may retract and the muscle can gradually undergo fatty degeneration, making later repair more challenging.
Common Symptoms
Many athletes ignore early warning signs.
Typical symptoms include:
Persistent Shoulder Pain
Pain is usually felt deep inside the shoulder and often radiates down the outer upper arm.
Pain at Night
One of the hallmark symptoms is difficulty sleeping on the affected side.
Many patients wake repeatedly because of shoulder discomfort.
Weakness
Players often notice:
- Reduced serving speed.
- Difficulty hitting overheads.
- Weakness lifting the arm above shoulder height.
- Trouble fastening a seatbelt or reaching behind the back.
Clicking or Grinding
Some individuals experience:
- Popping.
- Catching.
- Grinding sensations.
- Pain during certain arm positions.
These symptoms may indicate tendon irritation or associated shoulder impingement.
Why Tennis Technique Matters
Rotator cuff injuries are not caused by serving alone.
Several factors increase stress on the shoulder:
- Poor serving mechanics.
- Weak shoulder blade (scapular) muscles.
- Tight posterior shoulder capsule.
- Inadequate warm-up.
- Excessive match volume.
- Insufficient recovery between training sessions.
Modern sports medicine increasingly emphasizes correcting movement patterns rather than simply treating pain.
Diagnosis in the USA
Orthopedic specialists typically perform:
- Detailed medical history.
- Shoulder strength testing.
- Range-of-motion assessment.
- Special clinical tests.
- X-rays to assess bone structure.
- Ultrasound or MRI to evaluate tendon damage.
MRI remains the gold standard for confirming rotator cuff tears and determining their size.
Conservative Treatment: The First Line of Care
Fortunately, approximately 80–85% of partial-thickness tears and many small degenerative tears improve without surgery when managed appropriately.
Phase 1: Pain Control (Weeks 1–3)
Initial goals include reducing inflammation and protecting the injured tendon.
Treatment may involve:
- Avoiding painful overhead activity.
- Temporary modification of tennis participation.
- Ice after activity.
- NSAIDs such as ibuprofen or naproxen, when appropriate and recommended by a healthcare professional.
For severe pain interfering with rehabilitation or sleep, physicians may consider a corticosteroid injection into the subacromial space. Because repeated steroid injections can weaken tendon tissue, they are generally used selectively rather than as a long-term solution.
Phase 2: Restoring Motion (Weeks 3–6)
Once pain decreases, physical therapy focuses on restoring normal shoulder movement.
Common exercises include:
- Pendulum swings.
- Assisted range-of-motion exercises.
- Gentle stretching.
- Posterior capsule stretches.
- Shoulder blade mobility drills.
Maintaining mobility is important because prolonged immobilization can increase the risk of developing adhesive capsulitis (frozen shoulder).
Phase 3: Strengthening (Weeks 6 and Beyond)
As symptoms improve, rehabilitation shifts toward rebuilding strength.
Programs typically include:
- Resistance-band external rotations.
- Internal rotations.
- Rows.
- Scapular stabilization exercises.
- Lower trapezius strengthening.
- Serratus anterior activation.
Modern rehabilitation also emphasizes the kinetic chain, recognizing that efficient serving power begins in the legs and trunk rather than the shoulder alone.
When Is Surgery Recommended?
Not every tear requires surgery.
However, orthopedic surgeons often recommend arthroscopic rotator cuff repair when:
- A full-thickness tear occurs after an acute injury.
- The tear is large (often greater than 3 cm) with repairable tissue.
- Significant weakness persists despite rehabilitation.
- Pain and functional limitations fail to improve after approximately 6–12 weeks of structured physical therapy.
- The patient wishes to return to high-demand sports or occupations.
Early evaluation is particularly important for active individuals because delaying treatment for a repairable full-thickness tear can allow the tendon to retract and the muscle to deteriorate over time.
Sleeping Tips During Recovery
Many patients struggle more at night than during the day.
Helpful strategies include:
- Sleeping on your back when comfortable.
- Sleeping on the unaffected side.
- Placing a pillow beneath the injured arm to support the shoulder.
- Avoiding positions that allow the shoulder to roll forward.
Improving nighttime positioning often reduces pain and improves sleep quality.
Can Tennis Players Return to the Court?
Most athletes can return to tennis after appropriate treatment, but timing depends on the severity of the injury.
Many players with partial tears return after successful rehabilitation, while recovery after surgical repair generally requires several months of guided rehabilitation before returning to competitive overhead sports. The exact timeline varies based on the size of the tear, the surgical repair, healing, and the athlete's progress.
Returning too early significantly increases the risk of reinjury.
Prevention Tips for Tennis Players
Reducing shoulder injuries begins long before pain develops.
Sports medicine specialists recommend:
- Warm up thoroughly before serving.
- Strengthen the rotator cuff and shoulder blade muscles.
- Improve core and hip strength to reduce shoulder load.
- Gradually increase serving volume.
- Maintain flexibility of the shoulder capsule and chest muscles.
- Allow adequate recovery between intense training sessions.
- Address shoulder pain early rather than playing through it.
Final Thoughts
A rotator cuff injury can be frustrating for tennis players, but it does not necessarily mean the end of an active lifestyle or competitive play. Early diagnosis, appropriate rehabilitation, and attention to biomechanics allow many athletes to recover successfully without surgery. For larger or complete tears, timely orthopedic evaluation is important because early repair may improve the chances of restoring shoulder strength and function.
The shoulder is the engine behind every serve, overhead, and powerful forehand. Protecting it through proper training, conditioning, and prompt medical care when symptoms arise is one of the smartest investments any tennis player can make for long-term performance and health.
Medical disclaimer: This article is for educational purposes only and should not replace evaluation by a qualified healthcare professional. Persistent shoulder pain, significant weakness, inability to lift the arm, or pain following a traumatic injury should be assessed promptly by an orthopedic specialist or sports medicine physician.